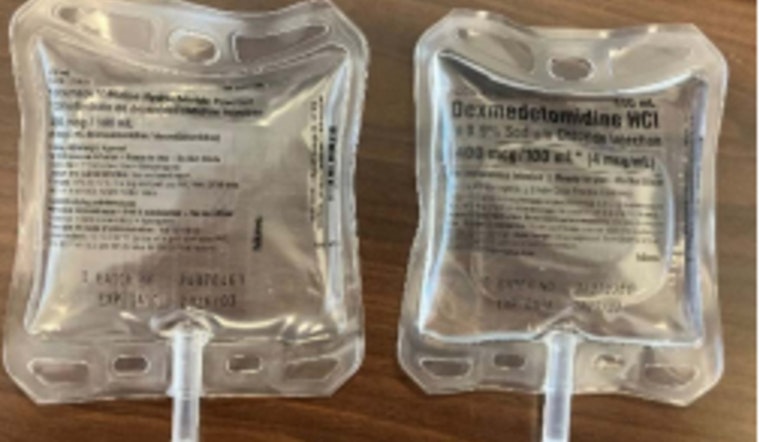
In what's being categorized as a significant medication packaging error, a nurse administered the wrong drug to a patient after a mix-up with infusion bags. The nurse, who was working off the information presented by the labeling on the outside of the drug packaging, ended up giving a patient dexmedetomidine instead of the prescribed acetaminophen. The Arizona State Board of Nursing (AZBN) reposted a report about the incident, wherein the report emphasized the severity of the packaging mistake. It was noted that the nurse scanned the barcode on the overwrap, which did not flag any issues, leading to the administration of the incorrect medication.
The error was only identified post-administration when the patient's expected relief from pain did not occur and instead, adverse effects indicative of dexmedetomidine use became evident, which was not what was intended when they went to the hospital. The report detailed how this oversight could lead to significant patient harm. The board has urged healthcare facilities and staff to double-check all medications before administering them and to report any similar packaging inconsistencies immediately.
Healthcare professionals are reminded of the importance of vigilance when it comes to drug administration. While the barcode scanning systems in place are generally reliable, they are not infallible, and this event is a potent reminder that technology must be augmented with human scrutiny. The incident has also prompted a review of medication handling and dispensing procedures in many healthcare facilities to prevent future occurrences of this type.
The AZBN has not released information regarding the patient's condition post-error or specified any disciplinary measures for the nurse involved but it has stressed that patient safety is of utmost priority and the incident serves as a critical learning opportunity for the healthcare industry. Institutions must prioritize ensuring that the checks and balances in the medicine administration processes are foolproof to avoid any repetition of such life-threatening mistakes. Further investigations into how the packaging error occurred are ongoing, and updates to protocols and procedures are expected to follow.
Editor's Note: An earlier version of this article misstated the source of the report. The report was originally from the Institute for Safe Medication Practices.









